 She's baaaaack!
She's baaaaack!
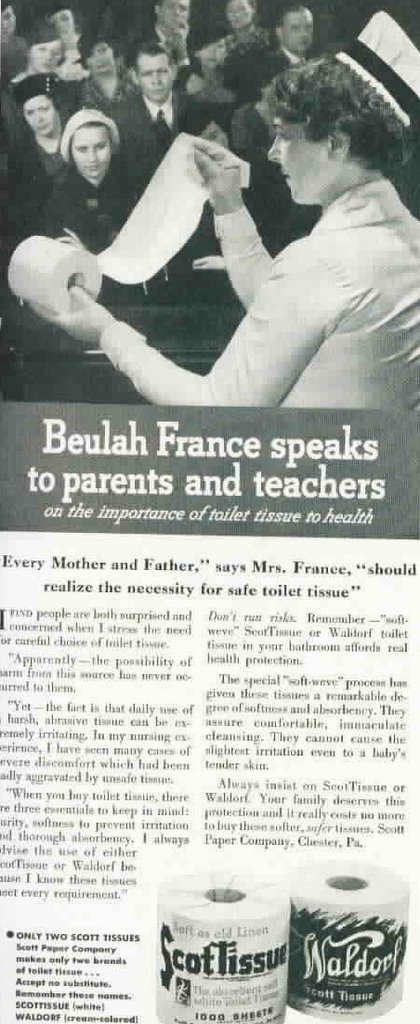
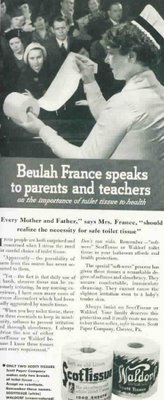
It's Beulah France, RN! Of New York!
The a nurse who made a career out of fondling toilet tissue.
The first nurse with an endorsement contract.
Now she is speaking to parents and teachers about the importance of toilet tissue to health.
Apparently it was no longer appropriate to use one's hands now that toilet tissue had been invented.
I'm trying to be delicate here.
Which is exactly the point!
If your toilet tissue is too rough it can irritate tender nether region areas.
Who wants to wipe with wood chips?
hhhhhhhhhhhhhhhhhh
Why am I blogging?
I don't mean that in a philosophical sense, I mean
why am I
blogging at 0133 am when I have a twenty-three page ACLS study guide sitting here on the end table.
And the class is Friday.
And it's only a recert class so I have to actually be prepared when I get there.
At least I was able to download the study packet.
Only to discover I have the same book that I just purchased.
They sure grabbed us by the gonads when they made certification mandatory. I paid about $150 for a five hour class. At least this company also gives you a BLS card, too.
And then somewhere along the line I realized that every four years my BLS, ACLS, PALS, TNCC and NRP are all due within
two months of each other.
BLS and ACLS are pretty self explanatory.
PALS (Pediatric Life Support) is also required by my facility, but it should be required at EVERY facility. You would be surprised at the number of ER nurses who are not comfortable taking care of kids with anything more than a virus. I'm not putting them down, it's just not an area they are comfortable in. The newborns with temps of 101. The tripoding, drooling epiglottitis
patient
(thank God I have yet to see
that). The lethargic two-year-old that should be screaming at everything you do, yet lays there and just
takes it
. The croup patient who is retracting to the point that his supraclavicular area is tapping his scapula. The sick ones.
(Just a note: I had a doctor once tell me to
never describe a pedi patient as "lethargic" in a chart, but to simply describe the behavior witnessed. Apparently "lethargic" is a trigger word when it comes to lawsuits. But that is true of most of nursing charting: you describe what you see, you do not label it - for the most part).
TNCC (Trauma Nurse Core Curriculum) is not required for employment at my facility, but stabbings and gunshot wounds don't always come in by ambulance. Sometimes they ar courteous enough to
walk through the entry portal. Or as I've noted before, they can be in an MVA and three weeks later their
spleen blows up. Trauma patients....they can sneak up on you like Dracula on a carotid. And lose just as much blood!
NRP (Neonatal Resuscitation) is also not required, but you never know when the only thing standing between you and a crowning head is....well....YOU!
Like the time a particularly assertive newborn pushed aside his mother's Victoria's Secret maternity undies and plopped on the floor. In the ER.
Or the time I stood there with a hand in a sterile glove watching the curly black hair of another little boy just one contraction short of landing in my hand. Oh, I had plenty of helpers, but they were all standing five feet behind me because, as the actress Butterfly McQueen so succinctly put it in that grand movie so very long ago: they "did'n know nothin' 'bout birthin' no babies!"
Hell, neither did I. I just figured that millions of babies have been born and this one would be unique because it was
my hand that guided the head. I looked as cool as a cucumber and felt as calm as if I had an amp of adrenaline shot in my derriere. At the last minute the doc delivered the baby. It took me sitting down 20 minutes before my legs stopped shaking.
Hence, my wish to have NRP under my belt.
Alas, I am rambling. It is now 0206. I must study for my ACLS. I paid good money for it, I want my card!
hhhhhhhhhhhhhhhhhh
Oh, and for those of you who watch "American Idol" I have two things to say : (1) If I wasn't married, I would run off with Simon Cowell in a New York minute and (2) I have already picked the final twelve AND the winner of the contest so you can all save your votes and just enjoy the show. Thank you.
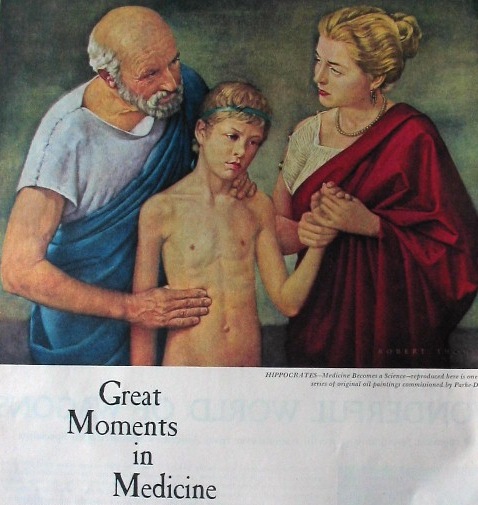 I call this composition "Homeless Man Diagnoses Appendicitis in ER Waiting Room With Mother Draped in Blanket While Child Freezes With Wreath on Head".
I call this composition "Homeless Man Diagnoses Appendicitis in ER Waiting Room With Mother Draped in Blanket While Child Freezes With Wreath on Head".