Ambivalent Compassion - The Migraine Sufferer
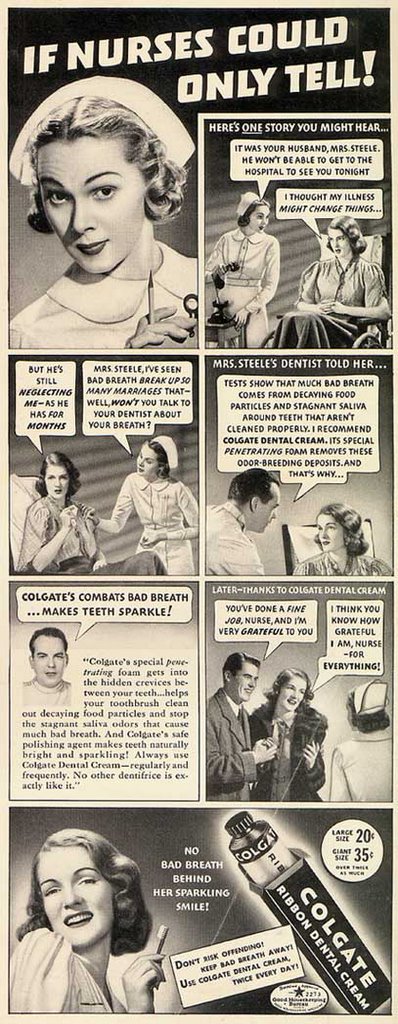 I wish the dialogue was visible on this ad for Colgate toothpaste.
I wish the dialogue was visible on this ad for Colgate toothpaste.
Wifey in gorgeous robe is upset because her husband pays no attention to her and not even her "illness" has changed his attitude.
Nurse Subtle informs Wifey that she has seen "bad breath" break up so many marriages.
Apparently Wifey's breath makes a cat-box smell like springtime in Paris.
Why, let's get a dental consult. Right here in the hospital.
Dr. Dental tells Wifey that her bad breath is caused by putrid, decaying animal flesh stuck between her teeth and saliva that's a-liva with bacteria. He prescribes Colgate.
Wife is shocked that she, of all people, should have to brush her teeth.
She tries the Colgate "dental cream". "Illness" cured.
And her marriage to her shallow, non-communicative husband who didn't have the cohones to mention her breath issue and won't even visit her when she is sick in the hospital is saved.
Much of the above dialogue was paraphrased by yours truly. But you get the idea.
Today's ads are Pulitzer-prize material compared to this stuff.....
hhhhhhhhhhhhh
Nowhere is this balance of compassion and cynicism more obvious than with caring for patients with chronic pain issues. For this post I will focus on the migraine patient.
I'm no stranger to headaches. Twice in my life I have known what it is like to feel like your head is going to explode. So, the first thing I do after assessing my migraine patient's color in the triage room is I turn out the light before I get the history, as most of the patients will suffer from photophobia.
I make sure they have a private room with the lights out whenever possible. Sometimes they have to wait a bit longer for the advantage, but I let them know why they are waiting.
For new patients I ask them what has worked in the past. Some don't know, others can recite specific dosages. I ask because if they know, it saves a lot of time and the need for re-dosing. If a patient states that it usually takes 100mg of Demerol, IM, to take the pain to a tolerable level it seems silly to give it in 25 mg increments. Oh, the doctors can order it that way, but (1) trust me, it will NOT work until the usual dose is reached and (2) the patient stays longer in the ER because of the need to re-evaluated after every administration of the med.
Hopefully the doctor has given them prescriptions for pain at home. I make sure the patient has a ride home. I have bad feelings about putting a female patient under the influence of a narcotic into a taxi, although they will often insist it is their only way home.
And this brings me to the cynical side of my migraine ambivalence.
I've been burned.
- I had a patient appearing very ill (headache, vomiting, photophobia) and placed directly into a room. It was discovered that just an hour before, said patient was at our "sister" ER and both departments worked off the same computer system. All it took was one phone call to ascertain that the patient had received enough narcotics to allow him to have floated to our facility. Well, he just floated back home without anything from us!
- Sometimes a nurse will work in more than one facility. One of my patients was identified as having been at another facility already twice that week for the same complaint: migraine. I believe I already told the story in another post that related a nurse traveler who recognized a drug seeker from the east coast while working here in CA.
- There are the patients who take the taxi, drive around the block and then get in their car and drive off. I know this happens because the taxi drivers come back and tell us the patient only went to the corner and then got out of the taxi and walked back up to the parking lot.
- If "New Miracle Drug" comes out on Wednesday and the patient states he is "allergic" to it on Friday, it usually means that somewhere, somehow the patient received the medication and it didn't work. Saying there is an "allergy" to a medication is one way an illegitimate drug seeker will keep from getting that drug.
If you are a patient with a chronic/recurrent migraine issue:
- Carry with you a letter from your neurologist outlining your treatment plan, discussing what to do in a case of breakthrough pain and gives medication/dosage recommendations. Make sure it is updated often, in other words, don't bring a letter dated 2000.
- Bring a list of your medications and allergies/reactions with you. The apex of a migraine is no time to be trying to think of your medications. Keep it in your purse/wallet.
- Bring your ride home with you. Don't take the chance you'll be medicated and have no way to get home. Don't drive yourself to the ER when you are in that much pain, it isn't safe.
- If you are certain that your pain is unmanageable at home with what you have available, it may be worth placing a call to your doctor. Often, they will call ahead to the ER so that we are expecting you. They may even talk with the ER doctor to discuss your case and treatment options.
There is a line in the movie "Ghostbusters" that shows the guys in a TV commercial saying, "We are ready to believe you!"
We are ready to believe you here in the ER, too.
But trust me, we can spot a phony a mile away.
posted by Kim @ 1/19/2006 12:23:00 AM
25 comments
![]()
![]()











25 Comments:
With all that you know, I bet you can.
that's the best ad you've posted yet... omg!
Once we had three seekers come in at once. If they hadn't been discussing their 'stories' in the waiting room, it might have worked out better for them.
And last weekend, as she was leaving AMA, a seeker's sister told us that they had been to every ER in the city, getting xanax prescriptions. You can imagine how livid the ER doc was!
Have I told you lately how much I love your posts?
Gee, you have to be a detective too?
That would explain why, about 3 years ago, when I went to the Er for a severe migraine, I was treated with disdain and the nurses were SO not nice to me.
I have a long history of migrainses (as do both of my daughters) but I am also allergic to EVERY anti-inflammatory on the market. So I guess my claim of a headache combined with allergies to medications rang warning bells to them.
I can certainly understand the need to weed these people out but it really does make it tough on those with legitimate issues.
Dawn
Dawn,
Being allergic to NSAIDS would not have been a trigger, at least to me. If you are allergic to any oneof them, you would never be given any of them due to the possibility of a cross reaction.
I'm like the soup nazi on Seinfeld, except I'm the NSAID nazi - allergic to aspirin? No ibuprofen for YOU!
And you know what, even the people I KNOW to be drug seekers I treat with respect and kindness. The fact that they are seeking drugs is an illness in itself. Some nurses are just mean, period, headache or no headache.
I used to get whopper headaches every single month, cycle related. They were never diagnosed as migraines, but they shared many of the traits. If I caught it immediately (and I mean half an hour) with ibuprofen I was okay, but if I let it go I was in agony. Sometimes I had Vicodin in the house and thank god that worked for me.
If only drug seekers would read your column and take your advice. If only they had morals and bought their drugs from the corner dealer, like everyone else. It sure would make life easier for us migraneurs who really do need help and often don't get it at the hospital. Most migraneurs I know don't and wouldn't-if-their-lives-depended-on-it, go to the hospital.
One other thing I've learned is that when I'm having weeks where I feel like I have to go to the ER more than once that week, because that does happen to me, it's usually because I'm starting a cluster headache cycle ontop of the migraine cycle, OR because the doc in the ER didn't believe me when I said this amount of medication will fix me right up and take me out of pain, so he gives me much less and sends me home, still in pain. Again, all this learned from battleworn experience.
Thanks for insight from the other side of the needle. :) I still can't believe that drug seekers go to the ER to get drugs. That just totally blows me away--and that that happens often is even more mind-boggling.
The funny thing is that at times when I've been in the throes of agony, I've wished I knew whoever the neighborhood drug dealer was, because it would be much less of a hassle to get the meds I needed from him rather than go through the whole ER experience. I guess that's why I can't imagine why anyone would subject themselves to such humiliation and waiting around for hours for treatment. I don't get that.
Love your interpretation of the ad, btw, that's hilarious. Thank you so much for posting about this. It did my heart good, tonight, to see your post. Very well done. Brava! Again, great post and totally spot on. Thank you, on behalf of all your migraine patients, THANK YOU. Wish I could give you a big hug and smooch for treating your patients, all your patients, professionally and with dignity. That's how it should be. :) (sorry for writing so much)
Jess
PS. Do you want to write a Carnival of Compassion blog entry? I think this particular entry would be perfect, absolutely perfect! And, it will bring more readers to your site, too. Let me know if you'd like to participate by following the link at the bottom of the page. Check it out here: http://www.medsim.net/carnivalofcompassion.php
Jess
In the local context, people fake 'migraine' more for medical leave than drug fixes (it being harder to prove that someone does NOT have headache).
We think 'addict' when someone professes an intractable cough that 'can only be relieved by Procodin'.
BTW the dialogue is easily readable if you click on the ad for the enlarged version. Although, I think if I told my patients "WON'T you see your dentist about your bad breath?" they'd probably just start crying and yelling for their mummy...
Loved the post and wish that it wasn't so- it really seems like the good people are the ones who suffer in such a big way. My B-IL is an ER nurse and has told me about a seeker that went 600 miles and hit every hospital on the route- that is COMPLETELY different than the person with documented migraine isssues that are related to a triger like menstrual cycles, etc.... He still thought it was right, or at least understandable, to treat all migraine sufferers with the same suspicion. A bit jaded, and so unfortunate.
The thing is, there are so FEW fakers and so many in need that it seems like a crime to say guilty before proven innocent, just because of the idiots. I should not have to say that the court system presupposes innocence, and when presented with proof, often acquieces to the truth. Doctors, who have promised to do no harm, often do not follow their own mandate. Harm, whether physical or psychological is still harm.
Chronic pain may be immeasurable, but it is not without consequence to the people who have it, and the people in their lives. Please do not forget that.
Thank you so much for having some compassion. I have been treated with suspicion a few times and it is so devastating. Interestingly enough, the one time I was drilled was because I was able to tell them what I needed. They looked at me like a druggie. It was awful. Tried to treat me with advil. LOL
Anyhow, I really appreciate your comments. It gives us all some hope that the ER doesn't have to be an inquisition.
I have had migraines for 24 years....so, I know what works and I know what doesn't. People like you give me hope.
i need more years of experience. i still can't spot a phony even if he is breathing at my neck and literally making fun of me. i have this voice in my head that keeps telling me: "pain is subjective". i just say a patient is a druggie if he/she says so. well, everyday is a day to learn something new.
My anaesthesia professor once said: nobody ever died of pain.
I bet HE never had migraine. :)
I had serious migraines that stopped when I addressed other issues in my life. I realize that this doesn't work for everyone, but doctors need to do more than just address the current pain . . .maybe it isn't medication that is needed.
There are many of us chronic migraine sufferers out here who are pretty much treated like the worst slime to ooze out from under a rock every time they go to an ER for help. And I'm talking about ERs all over the US, so this problem seems widespread.
Perhaps you can tell the difference between a person just trying to get loaded and a person in desperate need of pain relief. But many of your colleagues can't or won't.
If you are interested and it seems like you are, I suggest that you take a look at the website
http://www.migrainepage.com/cgi-bin/dcforum/dcboard.cgi
where you can read about what we really go through, some of us on a daily basis.
Love the ad. Makes me want to brush, at least right now, possibly q4h.
Thanks for linking my blog to yours - I appreciate your kind comments and will start checking in on you routinely, also.
Anonymous, I visited and I linked to "The Migraine Page" here on the blog (couldn't link to just the discussion forum for some reason). Very interesting insights into chronic pain.....
I really appreciate it your article. I had a very nasty experience at the ER room I use. I get suffer migraines and sometimes I have to go to the ER twice a week. I go to the same ER room everytime to make sure all my records are in the same place. Also, to avoid being pegged as a drug seeker. I have a letter from my Dr. stating I suffer from migraines. Unfortunately, I've found that doctors more than nurses are really bad at treating the migraine. Thanks for your blog it gives me hope
I have really severe migraines--I had one every day for about 16 months, until I gave in and started using a fentanyl patch. I still get one about 1-3 times a week. And I've tried everything--pretty much every drug there is for preventatives, I've taken it. Currently on 2 anticonvulants and a calcium channel blocker, and before the fentanyl, that was still really not working--migraines every day, etc. Let me tell you, nursing school and working in a hospital with a migraine is a tough one!
I've been lucky to get really good doctors--my neurologist is a migraine specialist--but I have had some really bad experiences. Someone on the on-call neuro service called me crazy(As in, said to another person in the room, while I begged him for something to make that night's pain go away, "This is the craziest patient I've ever talked to."). When I go to the ER(I had to go a few weeks ago, after managing to stay out for a year...damn!), it's such a mixture--some people treat you like absolute shit("Where do you get your drugs? Why are you on fentanyl?" Talking in a booming voice, etc), some people are so sweet(Private room, lights out as much as possible, etc). And I go to the ED in the hospital I work at--would hate to see what the patients who don't have "Hopsital Employee" written across the top of their chart get treated like.
Wow. A novel there. Sorry to hog your comments section--Whenever someone talks about migraines on their blogs I usually try to jump in to tell my story and/or clear things up--hell, even I was biased against pain patients before this happens. Now, they're some of my favorite people to work with--the interventions really feel like you're doing something, ya know?
Thanks so much for this post. I've had migraine and CDH for 18 years.
I'm horrified by the ER stories that migraine patients share. But I'm just as horrified by the stories that nurses and doctors have about drug-seekers.
There clearly isn't an easy solution, but the tips that you've given are terrific.
Thanks for thinking of us and trying to make getting treatment easier -- for everyone involved.
Kerrie
www.thedailyheadache.com
I am both a migraine sufferer and someone who has worked on a suicide prevention hotline.
In my experience, chronic pain sufferers made up about 25-30% of our callers and were some of the most lethally suicidal I dealt with. (Bipolar patients made up another large group.)
I haven't gone to the ER for migraine, my experiences going there when I had gallbladder disease were so negative I haven't bothered.
I once read a dialogue among medical professionals about med seekers and some had the opinion that instead of always trying to weed them out from the real patients, why not just give them the pain meds? They reasoned that it's better to treat some who don't need to be rather than miss someone who legitimately needed help. Yes it doesn't feel good to be used in this way but since one doesn't always know, why subject legitimate patients to suspicion? The med seeker will get the meds somewhere, after all. Give it with a list of treatment programs if you must.
If a chronic pain patient can at least have temporary respite from pain, sometimes that makes all the difference in their will to live. Even taking it down a notch helps.
Kim,
In 2003 I suffered from Guillain Barre Syndrome with severe mylin sheath damage as well as axonal nerve damage. Because of that and the accompanying 6 months in bed four of it on the vent before I could learn to walk again I suffer from chronic pain. Currently it is being controlled by narcotics, but I can tell you, getting to this point where I am stable on my meds has been a challange. I have dealt with the "looks" and accusations of being a drug seeker and it really makes me angry. Some of these "compassionate" medical professionals didn't even bother to look at my medical history. What exactly am I supposed to do?
Quite frankly I am tired of cynical uncaring doctors and medical staff. Don't get me wrong, I have had many expieriences where they have been compassionate and it has touched me deeply. Many of those expieriences has come when I've been closest to death... on the vent and only half with it. But, I can assure you, one cynical burn out can ruin ten good experiences.
Also, the compassionate experiences had nothing to do with the administration of pain meds.
I am an ER nurse, and I use to have no tolerance for people who came in saying they had a migraine. Then I started having actual migraines, and I cn totally sympathize now with migraine sufferers, and I treat them a lot better than I use to. I had no idea how painful it was. It makes me a little better a weeding out who is just there for a fix, and who is really in pain.
Post a Comment
<< Home