What's In YOUR Pocket?
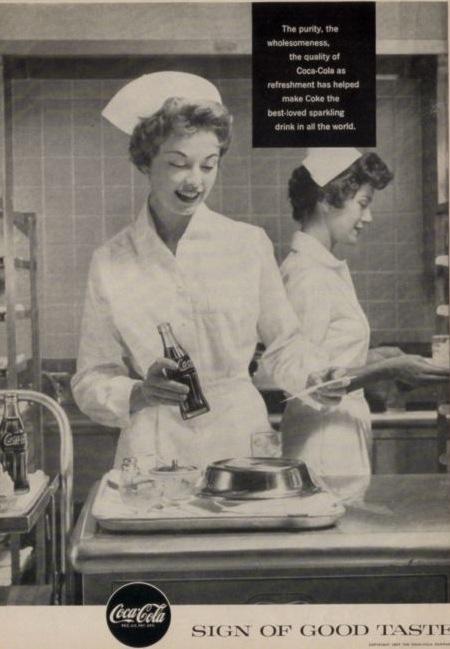
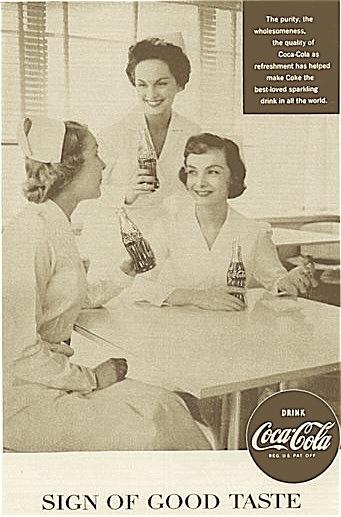
 Ladies, do you love your undies? Is your bra healthy for your budget?
Ladies, do you love your undies? Is your bra healthy for your budget?
Are you glad you can stop ironing your unmentionables? I have no doubt that this ad would engender massive amounts of protest if attempted today. Of course, the bra would be an underwire push-up, the bottom would be a thong and the model would be Shakira in a nurse's cap with a navy blue cape. Of course, they can't be sexist so there would be a companion ad with Justin Timberlake extolling the virtues of STAT-n'-Strap, the jock strap made for the guy who's MAN enough to wear the title, NURSE!
Ahem....Aside from underwear, there is more to dressing for work than just putting on the uniform. What about all the adjuncts you need to be at your peak efficiency? The tools of the trade? The building blocks of patient care? Let us discuss these various items.
- Your ID - you know, the plastic badge with your name on it in big, bold letters. Taping a photo of Catherine Zeta Jones over your photo is not allowed. I tried. It is common knowledge that ID cameras add fifty pounds. They do so!
- Your stethoscope - You will occasionally be seen to grope at your chest, wondering where it is. You get so used to wearing this that one day you forget to take it off at work and will wear it into the grocery store. You listen to your coughing child's breath sounds and go to basketball/soccer/volleyball/football practice with it dangling from your neck. You will do this. At least twice.
- In your right pocket:
- Scissors. Not those dainty little silver "bandage scissors" that fit so neatly into the little pocket organizer you will never use and couldn't cut the tip of a Barbie glove. Puh-lease! I'm talkin' big ol' trauma shears that will cut through leather. These go in your right pocket with...
- A tiny calculator. For when the doctor orders 1/748th of the dose you have on hand.
- Tape. Also in your right pocket. With a tiny fold made on the end so you don't have to pick at it, especially since they said you can't wear acrylic nails anymore and you are a chronic nail biter and can't get the tape to unroll naturally and it's such a pain and...but I digress.
- Notepad. Also known as a paper towel, upon which you have written the last set of vitals for the patient in 8A, the results of the urine dip in room 10 and the repeat pain measurement of the patient in 8B who was discharged 30 minutes ago but you haven't had time to chart it yet.
- Three quarters, a dime and two pennies that you got as change for your coffee on your way in to work.
- Two Hershey's kisses from the candy dish at the nurses' station, still wrapped but smooshy.
- In your left pocket:
- Your precious pens!
- Your wonderfully smooth writing, gel-based, royal blue Uniball writing utensils, so associated with you that, if found, they are put in your box.
- A red pen to mark orders you have completed on the doctor's order sheet.
- A black Sharpie. Because no nurse should ever be caught without a Sharpie. Their uses are too numerous to list here. Let's just say that the one time you don't have it, you will need it.
- Little plastic thingys that have your hospital's code system, fire system and Mission Statement written on them for easy reference. They are supposed to be on your nametag but they always fall off.
- One Hershey's Kiss. Wrapped and smooshy.
- Your Palm Pilot. Until it drops out the second time and you go put it back in your purse.
- On your shoes - shoe covers! Goodness only knows what you're walking around on in an Emergency department. Blech!
If you have a body like Shakira.......
posted by Kim @ 9/30/2005 08:49:00 PM
5 comments
![]()
![]()